Narrative medicine aims at removing the “noise” in healthcare communication, in an attempt to reach an understanding of the real feelings, thoughts, and wishes of patients. What is this noise? It is related to technology. Reliance on technology – beneficial though it undoubtedly is (provided it is used appropriately and effectively) – may become a Pavlovian automatism when healthcare providers are not able to talk and listen effectively to their patients. Assessing the language spoken during medical visits, what we often hear is technical jargon, a consequence of science and technology invading our daily lives. This jargon is linked to the Kleinmann [1] concept of “disease” as a biomedical object: when something is broken or goes wrong in or inside the body, the latter becomes an object for the healer, and whatever it is that is broken should be repaired, adjusted back towards normalcy. The idea of going back to normalcy implies acceptance of the principle that, in biology, organic laws rule human beings. However, the most recent research has successfully shown that this “normalcy” is not as narrow as we used to assume; instead, there are many possibilities of adaptation, both through genetic and epigenetic procedures, a view that has been captured by the concept of biodiversity.
From the patients’ point of view, on the other hand, “repairing the broken part” is quite simply not enough. Patients are human beings with inner feelings, whose actions are often dictated by those feelings. Physicians and nurses have to understand that, parallel to the ongoing “disease” or condition, they need to address and somehow gain the upper hand against emotions such as fear, sorrow, anger, and disgust, thereby moving from these “negative” sentiments back into a world of hope, serenity and peace. One way of doing this – perhaps the only way – is to rely on relatively simple language rather than jargon; this could well be the key to controlling emotions and establishing a useful relationship of care. However, as a general rule, the definitions that, during their training, medical and nursing students, on the one hand, and science and psychology students, on the other hand, learn for many types of disease are usually very technical, barely meaningful, and sometimes far away from true life experience, which is perhaps the biggest pitfall of all.
I have been wondering about the benefits that the use of more intelligible and realistic language, instead of jargon, could have for patients and doctors alike. In that respect, meeting Anna Wierzbicka, a Professor of Linguistics, and the founder of the Natural Semantic Metalanguage (NSM) [2] approach (together with Cliff Goddard), was an eye opener for me.
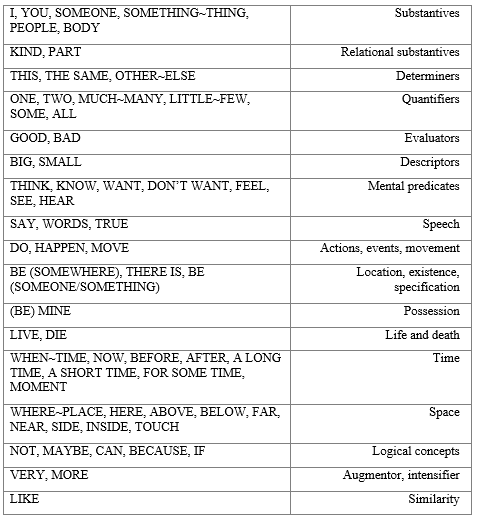
NSM is based on empirical evidence that there are sixty-five simple concepts (the “primes” or atoms of meaning) that can be expressed in all languages of the world. Using English words (since this essay is written in English), let’s briefly spell out some of these semantic atoms that are present all over the globe: before, now, moment, after, feel, think, say, do, know, happen, hear, see, touch, want, don’t want, big, small, good, bad, something, someone, body, you, I, people, mine, kind, can, maybe, if, inside, live, die. Personally, I find the fact that these words are alive in all spoken languages exhilarating. It provides me with a sense of belonging, not merely to a group of people, but to the human species, to humankind; at the same time, it gives me a sense of political spirituality, whereby, somehow, I become a citizen of the world.
How does all this fit in with Narrative Medicine? We as human beings are subject to the biological laws of life and death: we start out small, become big (i.e. grow up), live and communicate (i.e. say things to other people), get old and ill, and die. Nobody escapes illness. Nobody escapes death. All people can feel good things and bad things. People do not want bad things to happen to them; they want good things to happen. Such language deconstructions, which bring us right back to the Natural Semantic Metalanguage, are not a simple matter of playing with language, but relate directly to daily life and daily care.
One of the challenges when collecting illness narratives is choosing the proper tool for the oral or written interview. We can either opt for soliciting free-flowing stories without guiding the story-teller in any kind of way, or we can provide a guided series of prompts, which unfold diachronically from “the falling ill” to “the being ill”, up to “future expectations”. At the Fondazione ISTUD, we use both methods: unrestricted narratives that provide each of our patients with total freedom to tell his/her own story, but also the guided plot. We use the latter because we are committed to having an effective process that uncovers from start to finish, without omitting anything of importance, how a person copes with changes affecting the body or the mind (or both), how that person experiences the treatment or cure from the very early stages, and how his/her life changes at all levels, taking into account the people close to him/her, at home, at work or when engaging in social activities. The issue, here, is to collect narratives using the most understandable words, not only across different languages, but also across individuals who speak the same language, to avoid biases of “closed prompts” and “misinterpretation”. This is the reason why we developed a collaborative research programme involving the Australian National University and Fondazione ISTUD; its aim is to establish a dialogue between Narrative Medicine and the Natural Semantic Metalanguage approach, thus founding a new way to listen to patients’ thoughts, feelings, and actions when coping with the “illness”, or in other words, using NSM primes, the “bad things we do not want to happen in/inside the body”. An illness plot was written using mostly Natural Semantic Metalanguage – the universal words – and a few so-called Minimal English words – semi-universal words such as doctor, home, work, and scientific words such as specialist, nurse, which, as a result of globalization, are now presumably understood in a similar way in all countries of the world. [3]
Looking beyond our current use of NSM in collecting patients’ narratives, we can see other fascinating and useful applications of the metalanguage. One of them relates to the definition of illnesses from a patient’s rather than a doctor’s point of view. In recent times, looking at the definitions given of particular diseases, for instance in documents such as DSM-5 [4], the “bible” psychiatrists rely on for the definition of mental diseases such as depression and anxiety,. At a recent NSM workshop in Canberra, Australia, on March 17 and 18, Professor Wierzbicka shared some of her insights into the criteria DSM-5 uses to diagnose depression. One of them is “feelings of worthlessness or excessive or inappropriate guilt (which may be delusional) nearly every day.” Wierzbicka claims that no patient, even in the most technological and technocratic country, would ever say anything like this. I fully agree with her. The best way to talk to a depressed person is not by asking questions such as: “Do you feel worthless?” Questions such as these miss the point, as they relate to an external or outside perception of sickness and are unable to address what is inside the patient. A much better question to ask is: “How do you feel?” This question could be the start of a real conversation about depression, based on patients’ individual answers. Even if some patients – those who suffer from a medical condition called alexithymia, where there is no possible perception of feeling inside – might reply “I don’t feel anything”, a conversation can still get underway. The question “Do you feel worthless?”, on the other hand, is quite literally a conversation stopper.
Associating depression with feelings of worthlessness is taking it for something that is not related to personal and profound sorrow. The emphasis shifts away from the inner realm of the patient; instead of being an illness, depression becomes “a social event”, a sickness, a perception imposed from the outside. In other words, DSM-5 provides a definition that doesn’t focus on the nature of the illness, but unduly favours a societal perspective, namely that of a demanding society where all that matter is being productive, being a winner. This is a Kleinmann “sickness” approach: someone who is a loser, not able to do anything good, not worthy of belonging to the society of good performers, is “labelled” depressed. It is astonishing to realize that DSM-5 provides a “sickness” definition for depression, one of the most common mental illnesses, and that it relates depression to social failure, to guilt, to a moral judgement passed by others and imposed on the patient, whereas what it should do is describe what’s inside the patient. This is where NSM can provide good leads. Using NSM, Wierzbicka tells us the kind of words a depressed patient is likely to use: “I can’t do anything, I can’t do anything well”. And when the depression becomes really severe: “I don’t want to live anymore”.
This is just one example of how NSM can be used towards improving the psychiatric formulations in DSM-5, replacing them with more accurate and realistic formulations that are certain to create better channels of communication between carers and patients. Let’s consider another example: the definition of intrusive thought, which is at the basis of Obsessive Compulsive Disorder (OCD). Intrusive thought is based on “unwanted memories” (often related to a trauma), “violent thoughts” (where someone imagines doing violent/aggressive things), and “sexual thoughts” [5]. Through the narratives we have been able to collect from many patients, we have been able to identify intrusive thoughts that can be very different from the above. Personally, I think the DSM-5 list of intrusive thoughts is quite short. Unwanted thoughts can arise from fears of an undefined future – anxiety –, moral judgement of oneself and others, fear of poverty, fear of disease without any underlying trauma, lack of trust in the society, and many, many other possibilities, all of which can be summarized in NSM via the statement “I do not want to think about some kinds of things; when I think about these kinds of things, I feel something bad”. As for the widely used word anxiety itself, from a patient’s perspective, using a first-person perspective, it could be paraphrased as follows: “I don’t know what will happen to me after this; very bad things can happen to me; I don’t want this”. Taking the simplicity and universality of NSM seriously, a doctor could avoid falling into the trap of asking the patient: “Do you have unwanted memories? Any violent thoughts? Any sexual thoughts?”. There are myriads of unwanted thoughts in the different cultures of the world, whereas the intrusive thoughts that are the focus of DSM-5 refer mainly to possible undesired social behaviours, again focused on sickness – violence and sex – without exploring the thousands of other unwanted thoughts in people’s brains that are at the basis of an illness.
To sum up, NSM is an enabling tool allowing us to understand ourselves and others using everyday words that really matter. This is as true in the health sector as anywhere else. By the way, true is also one of the semantic atoms for which there is a word in every language. [6]
Narrative medicine and Natural Semantic Metalanguage. The Canberra lecture at Australian National University, Maria Giulia Marini
Notes
[1] Arthur Kleinmann, The Illness Narratives: Suffering, Healing, and the Human Condition, New York, Basic Books, 1988.
[2] Griffith
[3] See Minimal English for a Global World: Improved Communication Using Fewer Words (Cliff Goddard, ed.), New York, Palgrave Macmillan (in press) – and in particular chapter 11, by Bert Peeters and Maria Giulia Marini, “Narrative Medicine Across Languages and Cultures: Using Minimal English for Increased Comparability of Patients’ Narratives”.
[4] Psychiatry
[5] Ocdaction
[6] A particular acknowledgment to Prof. Bert Peeters, who kindly reviewed this article.
This is breathtaking, and very exciting for the potential of bringing back an eloquent and well considered simplicity into patient care.
Understanding the full dimensions of a word as seemingly simple as “body” and “inside” might help provide focus and meditation to the iceberg that each word truly is and the meaning it holds. A dictionary of 65 words of care, each one a tip of an iceberg. Wow!
thank you so much for sharing this.
(I am an artist, patient, and founder of an organization that brings puppetry, metaphor and the performing arts into chronic illness care– THE BETES Organization.)
Pingback: Narrative Medicine and Natural Semantic Metalanguage: An Emerging Dialogue – Centre for Medical Humanities
Thank you. This is exactly what this 65 words are for.
They are the primes, the atoms, the keys to enter in communication with the whole world.