When we speak about a health care ecosystem, we mean the complexity of human beings and roles, as Health care providers, dedicated to give health, wellbeing and comfort to physical, psychological, social and existential uneasy of the patients and the caregivers. This can be achieved through narrative medicine: the listening to the needs of the people, within the realm of possibilities. The listening also to the needs of the doctors as persons and not just as roles. The juxtaposition process is asking us to keep in mind two or more things which might not converge at the same time: to include pluralities of view, not to use the scissors to oversimplify reality.
We are very aware that this world is polluted by hyper medication, with a quick and fix system, selling loud voice that there is a remedy for every discomfort. As Doctor Dulcamara in the Elisir D’Amore opera of Gaetano Donizetti sells his bottled cure-all to the townspeople, including love potions. His “elixir” – in reality is only cheap red wine –who people pays for it with all the cash at his disposal. And sometimes, by chance, it will succeed, especially with young people. But we know that this kind of Elixir might have a temporary placebo effect that will fade. Quick and fix does not apply to many kinds of situational discomforts.
Alignment in the listening to the needs of all the main “lives” of this ecosystem is warranted: sometimes it is achieved, sometimes not.
It was extraordinarily achieved in the first months of the Covid-19 age, those darkest days, going to February, March, and April 2020: in our survey, asking a definition for this unknown virus, the three main roles, patients, caregivers and doctors wrote with one voice: “a monster”. A monster means an aberration from nature, something hidden, invisible but lethal and terribly dangerous. The alignment was complete: apart from a few of deniers- the same people who denies the climate change- there was a global effort by everyone in this ecosystem: citizens respected the lock down rules, sometimes shielding themselves, doctors and nurses were risking their lives to “try” to save other lives without any elixir tool, and DPI were hand crafted when not available.
It’s only in the next months that this “monster” transformed itself into an enemy and that fight transformed itself in a political and institutional war: with the advent of vaccinations (wonderful discovery) however the application of Green pass unfortunately created the casts of the vaccinated, the caste of those people who were waiting for vaccination but they were at the bottom of the list, and the caste of those people who for medical reason or for denials did not believe in vaccination.
Moving away from COVID-19, let’s enter another topic, which might be also driven by the social pressure of our contemporary life: depression. Ninety-six narratives from Italian people with major depression (36), their caregivers (27), and psychiatrists (33) were collected.
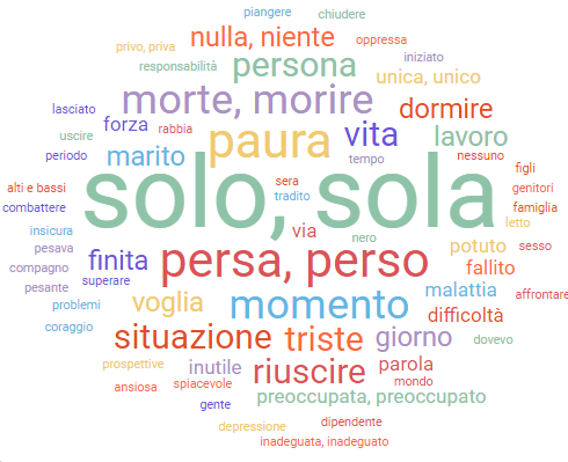
The word cloud from patients’ narratives, under the prompt “I was feeling”, gave the following picture:
The word cloud from doctors’ narratives, under the prompt “He/She (i.e., the patient) was feeling”, gave the following picture:

It is evident that doctors look at the patients more from an emotional point of view, using the Italian words “triste” and “tristezza” (sad and sadness). The existential problem is perceived by the caregivers in the words “senza vita”- “without life”, mentioning the fact that they are “without life” but not always by the doctors, who referred also to the “inadeguata” (inadequate) category, in the realm of the not being able to do. It looks like doctor are not always aware of the real condition reported in the patients’ words as solo – sola (lonely) and perso- persa (lost), being this situation, barely perceived by their caregivers, people who live close to them.
Beyond this, the words “morire- morte” (to die and death) are only written in the patients’ narratives and rarely in both the other points of view. The healthcare professionals, probably, not being able to handle the possible risk of suicide, replaced the words to die or death with “senza speranza”, hopeless.
From the caregivers’ narratives, the prompt “I was feeling” reported words as “impotente “powerless” or “inadeguato” – inadequate, showing the confusion and difficulty of living closely to a person affected by depression.
The collected narratives suggested that, while patients are in the “to be” dimension, as indicated by the words “solo” and “sola”, encoded in our cultural script of depression, carers are in the “to do” dimension, more based on “performance adequacy”, as in DSM-5 written by the American Psychiatric Association; this difference could explain the loss of reciprocal understanding, creating the feeling of loneliness.
This is a misalignment of which people curing people with depression should be informed: in this ecosystem while the patients whisper about loneliness or confusion the carers reply with not adequate and hopeless. Don’t’ we taste a mild bitter flavour of judgment? This ecosystem could be less at threaten while creating a better intimacy with the courage to asking questions as “Lonely, what do you mean by being or feeling lonely”? “Confused, in which sense?” “How could I help you? What could really help you” “Is there anything you might like?”.
And just listen to the words, maybe also the prolonged silence, also the silence has a sound. This will avoid quick and fix Dulcamara’s elixir, but will improve the alignment among the different livings in the ecosystem. Active listening and creative thinking for curing our ecosystem.
And if you wish now, you could read the Dulcamara’s aria:
DULCAMARA
Hear, hear, or rust;
Careful, do not breathe.
I already suppose and imagine
That as you know me
What a great doctor I am,
Encyclopedic doctor
Called Dulcamara,
The virtue of which preclaces,
And the infinite portents
They are known to the universe … and to other sites.
Benefactor of men,
Riparator de ‘mali,
In a few days I clear,
I sweep the hospitals,
And health to sell
For the whole world I want to.
Buy it, buy it,
I’ll give it to you for a while.
This is the odontalgic
Wonderful liquor,
Of mice and bedbugs
Mighty destroyer.
Whose certificates
Authentic, branded
Touch, see and read
I’ll do it to each one.
For this specific mine,
Sympathetic, prolific,
…
In a short week
More than a distressed widow
To cry ceased.
Or you rigid matrons,
Antiaging craved?
Your wrinkles are uncomfortable
With it you delete.
You want, damsels,
Well smooth to have the skin?
You, young gallant,
Forever having lovers?
Buy my specific,
I’ll give it to you for a while.
The paralytics move;
He sends the apopletics,
Asthmatic, asthmatic,
The hysterics, the diabetics,
Heals tympanites,…
You will tell me: how much does it cost?
How much is the bottle worth?
One hundred coins? … thirty? … twenty? …
No … nobody is dismayed.
To prove my happiness
Yes, welcome friend,
I want you, or good people,
A regal shield.